
Achilles Tendon Injuries
Achilles Tendon Injuries – Senior Podiatrist Matt Discusses
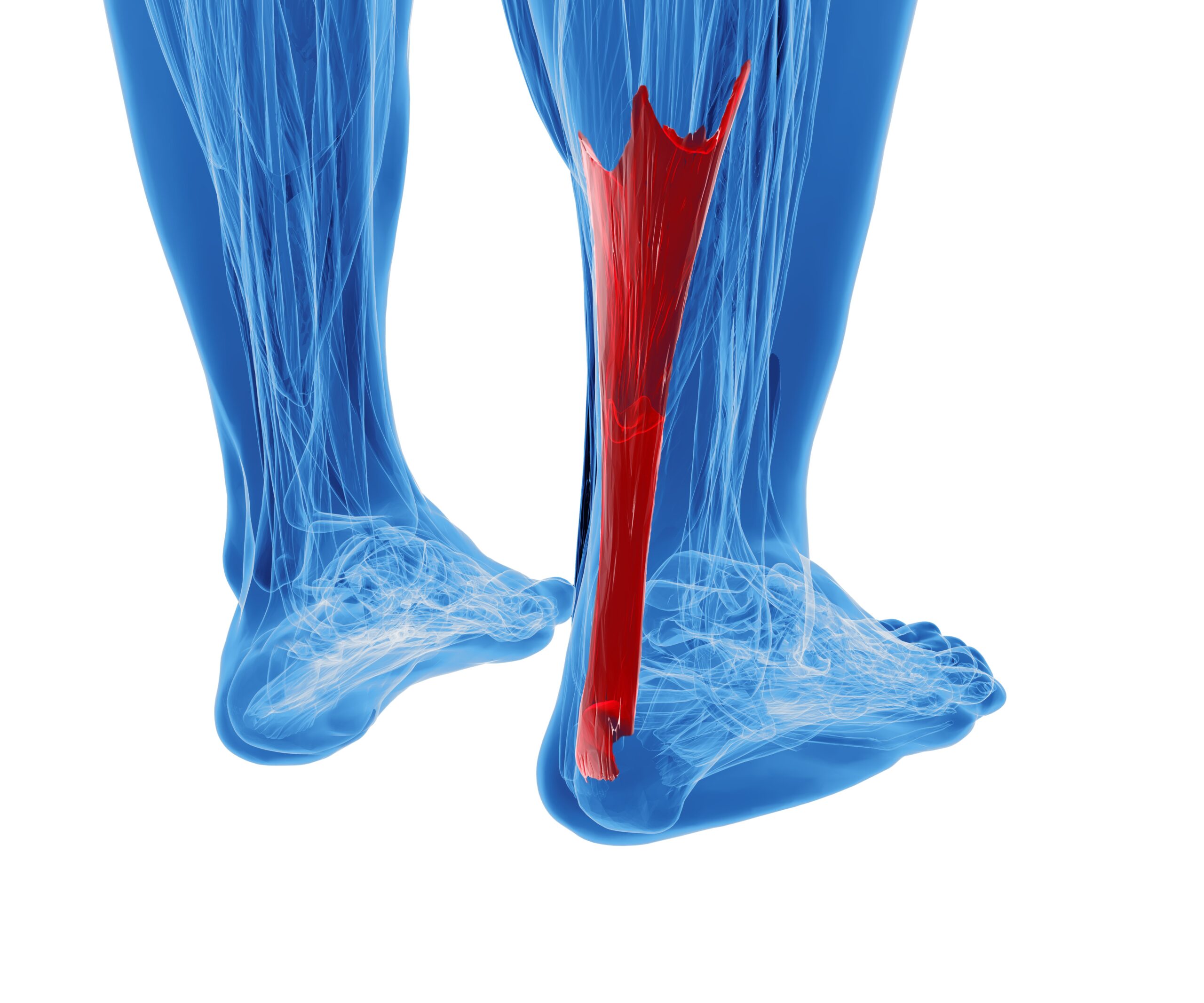
The Achilles tendon is the largest and strongest tendon in the human body. It is derived from a fusion of the Soleus, medial and lateral Gastrocnemius muscles. Its spring-like structure plays an important role in human movement by transferring forces generated by the Gastrocnemius and Soleus muscles (calf muscles) to the calcaneus (heel bone). The mechanical properties of the Achilles tendon, in particular its stiffness, influences force production and performance, and can also adapt in response to increases or decreases in mechanical loading. Due to its length and elastic properties, the Achilles tendon allows for energy storage and return during functional activities such as walking and running.
If we think of the Achilles tendon like an elastic band, in that a compliant less stiff tendon is like a stretchy thin elastic band, with greater stretch even with less force applied. They still return energy, but due to their increased stretch the recoil of the tendon has reduced speed and force. In contrast a stiffer Achilles tendon is like a thick elastic band they stretch less when a force is applied and recoil at a faster speed and force. These stiffer tendons provide more ‘free energy’ reduced ground contact time and improve overall running economy and speed.
During childhood the stiffness of weight bearing tendons such as the Achilles tendon has been shown to increase from the age of 9 years to adulthood. Age related increases in body mass and force production capabilities have been hypothesised to contribute to increases in tendon stiffness. Increases in body weight especially through teenage years will require tendons such as the Achilles to have a higher force production capacity, and will be partially due to increases in muscular strength through greater cross sectional area and an individuals ability to recruit and coordinate the available muscle mass for force production. Tendons should adapt based on their requirements to transmit higher forces form the muscle to the skeletal system safely and effectively.

As a requirement to tolerate greater loads a tendon’s stiffness is also dependent on its dimensions. As these dimensions change with age increases in tendon stiffness must also be set in the context of its growth. The ability of the Achilles tendon to cope with high loads (tensile strength) such as when running and jumping is related to its thickness and collagen content, with studies showing between 6-12 time body weight having been recorded in an adult human Achilles tendon when running.
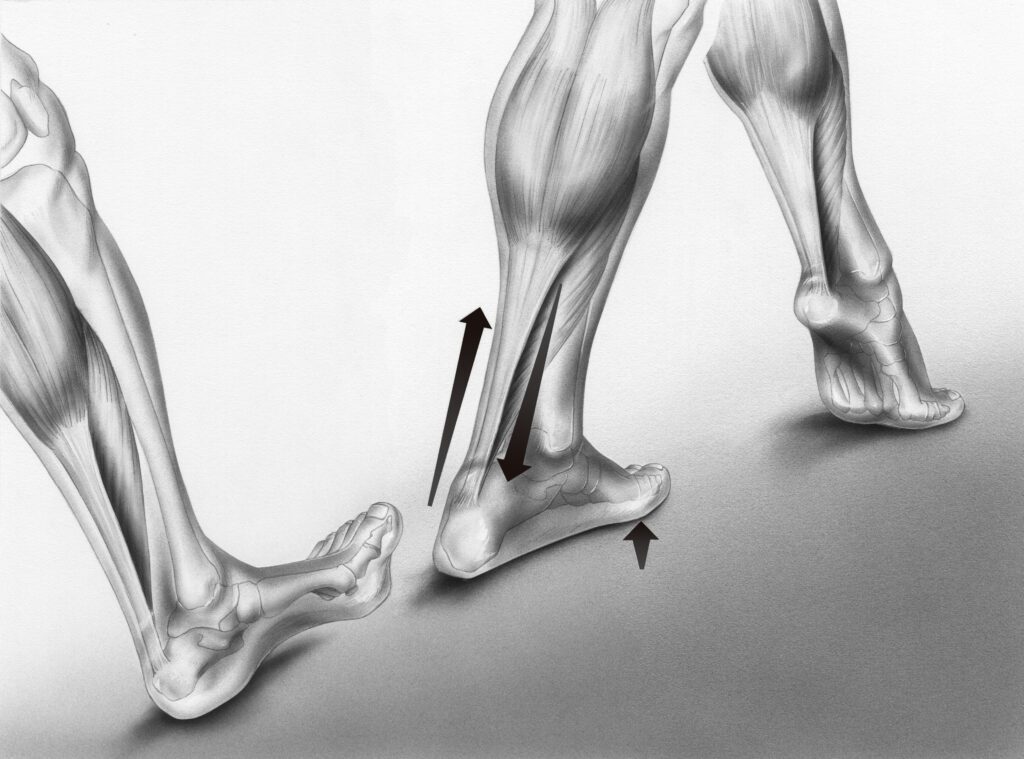
When running the Achilles tendon undergoes rapid lengthening and shortening during the stance phase of gait. This takes up the majority of the length change for the whole muscle-tendon unit, reducing the requirement for muscle fibre lengthening and shortening, minimising the muscle energy cost as the Achilles tendon is mechanically tuned to allow minimal muscle fascicle shortening during the stance phase with the majority of length change of the muscle tendon unit accommodated by the Achilles tendon.
When the Achilles tendon is cyclically loaded during running it may develop dynamic creep, resulting in greater length for a given load. If significant during or following a prolonged run, this would imply that for any muscle-tendon unit length and the same force requirement during stance, Achilles tendon elongation would be greater requiring greater muscle fascicle shortening. This additional fascicle shortening would require greater muscle work/energy and a higher shortening velocity.
Older adults walk slower with a higher metabolic energy cost than younger adults. Age related declines in Achilles tendon stiffness increase the metabolic cost of walking due to less economical calf muscle work and greater proximal joint work. As we age, reductions in ankle mechanical power during propulsion when walking occur and are often accompanied by compensatory increases in hip mechanical power.
The Achilles tendon and calf muscles interact to generate power via an energy storage (tendon lengthening and near isometric contraction of the muscles) and return (tendon shortening with muscle shortening over a slower velocity) mechanism, providing a more economical force generation. Some studies have shown that as we ages the calf muscles show short muscle lengths and greater Achilles tendon length when comparing older to younger adults. More recently a study highlighted that Achilles tendon tissue displacements in older adults were on average 63% more sensitive to changes in tendon force than those in younger adults. It is likely that as we age the reduced tendon stiffness in older adults disrupts the tuned neuromuscular interaction with the calf muscles, eliciting more tendon stretch for a given load.
Decreased tendon stiffness was found to be associated with decreased performance and may also influence Gastrocnemius and Soleus muscle fascicle behaviour. This would possibly increase AT elongation at a given force level making Gastrocnemius and Soleus muscle fascicles work at lower lengths and greater velocities, increasing energetic cost of walking and running. To overcome the decreased force generating potential with shorter muscle fascicle lengths an increase in muscle activation would be required in order to maintain muscle-tendon stiffness to the same level.
In a recent systematic review it was mentioned that a 25% reduction in Achilles tendon stiffness could decrease Soleus and Gastrocnemius muscle efficiency by 15%. As such, an increased energy cost and reduced efficiency potentially would lead to earlier fatigue, reduced performance and injury. With muscle attached to more compliant tendons it makes it more difficult to control the position of a joint spanning then tendon. Tendon elongation is accompanied by an equivalent shortening in the muscle. For a given contractile force a more extensible tendon will allow the muscle to shorten more. As the tendon lengthens due to reduced stiffness there is reduced muscular force.
Based on this it is vital that Gastrocnemius and Soleus muscle strength is maintained and developed to reduce the risk of fatigue related injuries of the Achilles tendon, especially when considering the Soleus muscle is the most dominant in running with a current paper showing that recreational runners should be able to perform a seated single leg calf raise (6 repetition max) at 1.5 x body weight. Based on clinical experience I have yet to see both highly competitive sports men and women or recreational sports men and women achieve anywhere near this target, suggesting many runners or sports individuals are at a risk of Achilles tendon injuries, based on significant strength deficits. Studies have reported that older adults that run exhibited a 10-16% stiffer mass specific Achilles tendon and a 7-10% better walking economy values than age-matched older non-runners, suggesting that older adults may be able to delay age-related reductions in Achilles tendon stiffness and increased metabolic cost in gait through maintaining strength and improved capacity to cope with the stresses from high impact activities.
Common Achilles Tendon Injuries
Non-insertional Achilles tendinopathy is a degenerative condition characterised by pain on activity. The location is 2-6cm proximal for the insertional at the calcaneus (heel bone). There are a number of risk factors that can contribute to this condition including:
– Increased Age
– Strength Deficits
– Training Errors (Running Mechanics/Increased Volume and/or Intensity)
– Biomechanical Factors (Reduced Ankle Dorsiflexion Range of Motion)
– Systemic Disease (Diabetes)
Management includes strengthening exercises for muscle adaptation and development such as heavy slow resistance training followed by improvements in tendon energy storage and recoil. Any biomechanical or training errors will need addressing. Ensure load management protocols are carried out to ensure tendon is not over loaded during rehabilitation and when maintaining fitness.

Insertional Achilles tendinopathy is a degenerative condition characterised by pain in the insertion of the Achilles tendon where it inserts into the calcaneus. It may be associated with irritation of the bursa or tendon sheath within the same region. Risk factors include;
– Biomechanical Factors (Reduced Ankle Dorsiflexion Range of Motion / Excessive Foot Pronation)
– Rigid Narrow Heel Counters in Footwear
– Slipping at the Heel in Footwear
– Training Errors (Running Mechanics / Increased Volume and/or Intensity
– Systemic Disease (Diabetes / Arthropathies
Management of this condition is difficult and takes time. Key is to reduce compression at the heel. One easy way to do this is through use of a heel raise in footwear along with ensuring footwear is not compressing or irritating the heel region. ICE can help form a pain relief view point and any biomechanical or training errors need addressing.
Current evidence shows that rest is not the answer and progressive load management is key. However it is important you get advice from a trained healthcare professional such as a musculoskeletal podiatrist or physiotherpaist to ensure correct diagnosis and risk factors are identified and addressed so that proper rehabilitation and management plans can be implemented for a safe return to sort.
Need help with your injury?
Click the button below to book an appointment with one of our HCPC Registered Podiatrists today!


Customer support
If you have any questions or need further assistance, we’re here to help. Feel free to reach out through our contact form or give us a call. Our dedicated team is ready to provide you with the support and information you need. Whether you're looking to book an appointment or have specific queries, don’t hesitate to get in touch.
Contact information
Official partners





Get in touch
